
Hand Hygiene: Shocking Statistics & How To Take Care of Your Hands
We’ve done the math on how many times nurses perform hand hygiene, plus some shocking facts and a few tips on how to take care of your hands as a nurse.
Our relentless research goes beyond shoes. Capsol allows us to talk all things nursing, from career advice and current news to self-care and mental health. These conversations with you, the community, and the world at large help us put our best foot forward when creating the best nursing shoes on the planet.


Thorough patient assessments are one of the cornerstones of good healthcare. As nurses, it’s imperative that we’re comfortable giving head-to-toe assessments and aware of all essential elements involved.
With great patient care comes great responsibility. As Antonia Villarruel, PhD, RN, professor and Margaret Bond Simon Dean of Nursing at the University of Pennsylvania was quoted as saying,
“Nurses are not just doers. Our work is supported by evidence and guided by theory. We integrate evidence and theory with our knowledge of patients and make important decisions with and for patients and families at the point of care. Research and practice are not separate but integrated. Nursing is a practice discipline with our own theories and research base that we both generate, use, and disseminate to others.”
Patient assessments are an essential part of any visit because it allows various components, needs, and problems being experienced by the patient to be notated and included in the approach to comprehensive care.
But just how do we ensure that patients are getting the most optimal care? It very often starts with thorough patient assessments, of which there are two main kinds:
For the purpose of this article, we’re going to dive head first into complete assessments.
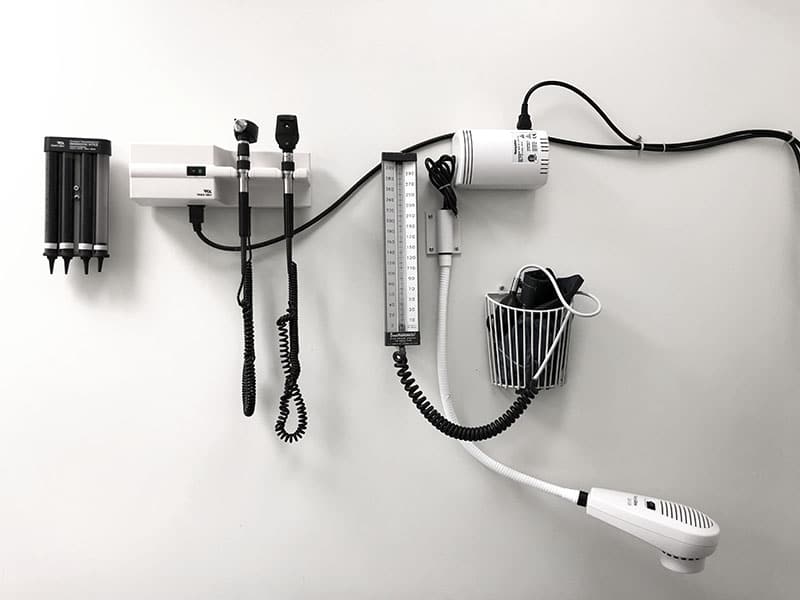
Let’s begin with the equipment and supplies needed to perform a standard thorough head-to-toe patient assessment (subject to change based on hospital and employer or situational requirements):

The way you approach conducting your assessment should be relatively the same every time. The main patient assessment goals at this time should be:
Vital sign measurement is essentially checking in on the body’s basic functions for any irregularities. Obtaining accurate patient vitals is imperative to ensuring accurate, corrective, and supportive patient care can be provided in relation to where base health lies and what it’s indicating is needed. When you’re doing a head-to-toe general assessment, the list of vitals that need to be collected can be pretty long. Here’s a list of what will most likely need to be gathered (assessments needed are not limited to this list):

Check head, ear, nose, and throat for sounds, color, appearance, and functionality
Following the completion of a head-to-toe assessment, it’s vital that any concerns or abnormalities are reported to coordinating physicians or other healthcare providers as needed. While patient care often begins with thorough assessments, coordination amongst staff and various departments is essential to ensuring the patient receives treatment and support for continued and improved health.

Author
most recent
We’ve done the math on how many times nurses perform hand hygiene, plus some shocking facts and a few tips on how to take care of your hands as a nurse.

Celebrate Pediatric Nurses Week as we talk about what pediatric nurses do, ideas for showing appreciation, and a breakdown of how to become one. Don’t miss this!

Ever wonder, what is with nurses and coffee? I mean, why do nurses love coffee? So many of us depend on that rich, hot java to jumpstart a shift.
0 Comments